Don’t let them forget it and vote
These days are precarious as Governors float the idea of martial law for not following “social distancing”, as well as they liked while they violate those same rules on national TV. Remember this tone is for a virus that has impacted 0.004% of our population. Imagine if this was a truly existential threat to our Republic.
The COVID-19 hysteria is pushing aside our protections as individual citizens and permanently harming our free, tolerant, open civil society. Data is data. Facts are facts. We should be focused on resolving COVID-19 with continued testing, measuring, and be vigilant about protecting those with underlying conditions and the elderly from exposure. We are blessed in one way, there is an election in November. Never forget what happened and vote.
Take that, Trumpkins!
I remain of the view that, based on what was and is known, Trump had no real alternative and ended up acting prudently.
Based on my reading of the data presented, a fair view is that--to anticipate my conclusion--Covid-19 is a very serious matter, but infection is far from an inevitability. Social distancing is warranted, but social isolation--to draw what I hope is a useful distinction--is probably not. That distinction may be useful going forward.
With that, we begin:
Against Panic
On a per-capita basis, we shouldn’t be panicking
...
Rank ordering based on the total number of cases shows that the US on a per-capita basis is significantly lower than the top six nations by case volume. On a 1 million citizen per-capita basis, the US moves to above mid-pack of all countries and rising, with similar case volume as Singapore (385 cases), Cyprus (75 cases), and United Kingdom(3,983 cases). This is data as of March 20th, 2020.
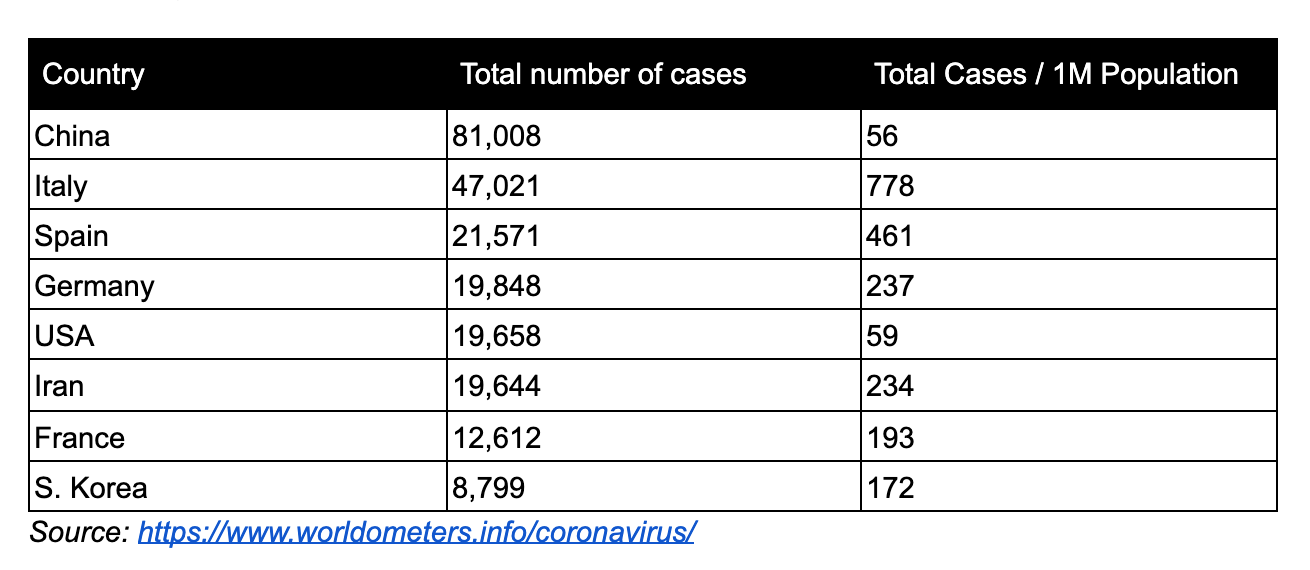
This suggests to me not simply that we're behind on testing--which we are, of course--but that the virus arrived here later than in other places. For reasons I can't explain. I say this simply from a seat of the pants view that if the virus had arrived here at the same time as in some other countries we'd have had a much larger number of serious cases presenting to hospitals than has been the case. That suggests that the US is taking strong measures at an earlier stage than other countries did, or that we may be on a par with Korea (based on other data).
The probability of catching COVID-19
The author calls this a "low" probability, but that's a relative term. It's better to compare it with the probability of catching seasonal flu. Seasonal flu is contracted by tens of millions of people every year. The number of people contracting Covid-19 would likely be some mix of "in addition to those contracting seasonal flu" and "people who contracted seasonal flu and are in a run down condition who then also contract Covid-19." Neither of those situations is a happy one if the rate of contraction of Covid-19 is similar to that of seasonal flu--which it is. Nevertheless, the numbers do also strongly suggest that avoidance is probably quite effective--and that perhaps we should be adopting higher measures of avoidance with regard to seasonal flu.
The World Health Organization (“WHO”) released a study on how China responded to COVID-19. Currently, this study is one of the most exhaustive pieces published on how the virus spreads.
The results of their research show that COVID-19 doesn’t spread as easily as we first thought or the media had us believe (remember people abandoned their dogs out of fear of getting infected). According to their report if you come in contact with someone who tests positive for COVID-19 you have a 1–5% chance of catching it as well. The variability is large because the infection is based on the type of contact and how long.
The majority of viral infections come from prolonged exposures in confined spaces with other infected individuals. Person-to-person and surface contact is by far the most common cause. From the WHO report, “When a cluster of several infected people occurred in China, it was most often (78–85%) caused by an infection within the family by droplets and other carriers of infection in close contact with an infected person.
From the CDC’s study on transmission in China and Princess Cruise outbreak -
A growing body of evidence indicates that COVID-19 transmission is facilitated in confined settings; for example, a large cluster (634 confirmed cases) of COVID-19 secondary infections occurred aboard a cruise ship in Japan, representing about one fifth of the persons aboard who were tested for the virus. This finding indicates the high transmissibility of COVID-19 in enclosed spaces.
Dr. Paul Auwaerter, the Clinical Director for the Division of Infectious Diseases at Johns Hopkins University School of Medicine echoes this finding,
“If you have a COVID-19 patient in your household, your risk of developing the infection is about 10%….If you were casually exposed to the virus in the workplace (e.g., you were not locked up in conference room for six hours with someone who was infected [like a hospital]), your chance of infection is about 0.5%”
According to Dr. Auwaerter, these transmission rates are very similar to the seasonal flu.
How is Covid-19 spreading in the real world? It's important to provide real world information rather than hypothetical scenarios.
Aerosolized Spread?
“This virus is not circulating in the community, even in the highest incidence areas across China,” WHO’s COVID-19 lead Maria Van Kerkhove said.
“Transmission by fine aerosols in the air over long distances is not one of the main causes of spread. Most of the 2,055 infected hospital workers were either infected at home or in the early phase of the outbreak in Wuhan when hospital safeguards were not raised yet,” she said.
True community spread involves transmission where people get infected in public spaces and there is no way to trace back the source of infection. WHO believes that is not what the Chinese data shows. If community spread was super common, it wouldn’t be possible to reduce the new cases through “social distancing”.
...
An author of a working paper from the Department of Ecology and Evolutionary Biology at Princeton University said, “The current scientific consensus is that most transmission via respiratory secretions happens in the form of large respiratory droplets … rather than small aerosols. Droplets, fortunately, are heavy enough that they don’t travel very far and instead fall from the air after traveling only a few feet.”
The media was put into a frenzy when the above authors released their study on COVID-19’s ability to survive in the air. The study did find the virus could survive in the air for a couple of hours; however, this study was designed as academic exercise rather than a real-world test. This study put COVID-19 into a spray bottle to “mist” it into the air. I don’t know anyone who coughs in mist form and it is unclear if the viral load was large enough to infect another individual As one doctor, who wants to remain anonymous, told me, “Corona doesn’t have wings”.
To summarize, China, Singapore, and South Korea’s containment efforts worked because community-based and airborne transmission aren’t common. The most common form of transmission is person-to-person or surface-based.
Surface Based Spread
COVID-19’s ability to live for a long period of time is limited on most surfaces and it is quite easy to kill with typical household cleaners, just like [seasonal] flu.
...
Presence doesn’t mean infectious. The viral concentration falls significantly over time. The virus showed a half-life of about 0.8 hours on copper, 3.46 hours on cardboard, 5.6 hours on steel and 6.8 hours on plastic.
According to Dylan Morris, one of the authors, “We do not know how much virus is actually needed to infect a human being with high probability, nor how easily the virus is transferred from the cardboard to one’s hand when touching a package”.
According to Dr. Auwaerter, “It’s thought that this virus can survive on surfaces such as hands, hard surfaces, and fabrics. Preliminary data indicates up to 72 hours on hard surfaces like steel and plastic, and up to 12 hours on fabric.”
Therefore, it's best to excercise caution when coming in contact with hard surfaces outside your home.
Geography and Climate
I don't believe we have data to support the author's contention that the change of seasons will mitigate Covid-19. It may, but it may not. It's presence in tropical areas like Singapore and Brazil or hot, dry summer areas (Australia) suggests that the mitigation would be temporary at best.
On the other hand, this now famous climate map illustrates that it does seem to spread most rapidly in a relatively narrow band (the green one). Unfortunately, it also illustrates that essentially all of Europe falls within that band, as do heavily populated areas of the US--New York, much of the Midwest, the Pacific Northwest:
How About Young People?
The data appears to show that those 19 and under are at a low risk for serious illness from Covid-19. However the data also negates, IMO, the authors belief that sending kids back to school is a good idea--young people are quite capable of spreading to those 20 and older:
According to the WHO’s COVID-19 mission in China, only 8.1% of cases were 20-somethings, 1.2% were teens, and 0.9% were 9 or younger. As of the study date February 20th, 78% of the cases reported were ages 30 to 69. The WHO hypothesizes this is for a biological reason and isn’t related to lifestyle or exposure.
...
However even if children and teens are not suffering severe symptoms themselves, they may “shed” large amounts of virus and may do so for many days, says James Campbell, a professor of pediatrics at the University of Maryland School of Medicine.
Children had a virus in their secretions for six to 22 days or an average of 12 days. “Shedding virus doesn’t always mean you’re able to transmit the virus”, he notes. It is still important to consider that prolonged shedding of high viral loads from children is still a risky combination within the home since the majority of transmission occurs within a home-like confined environment.
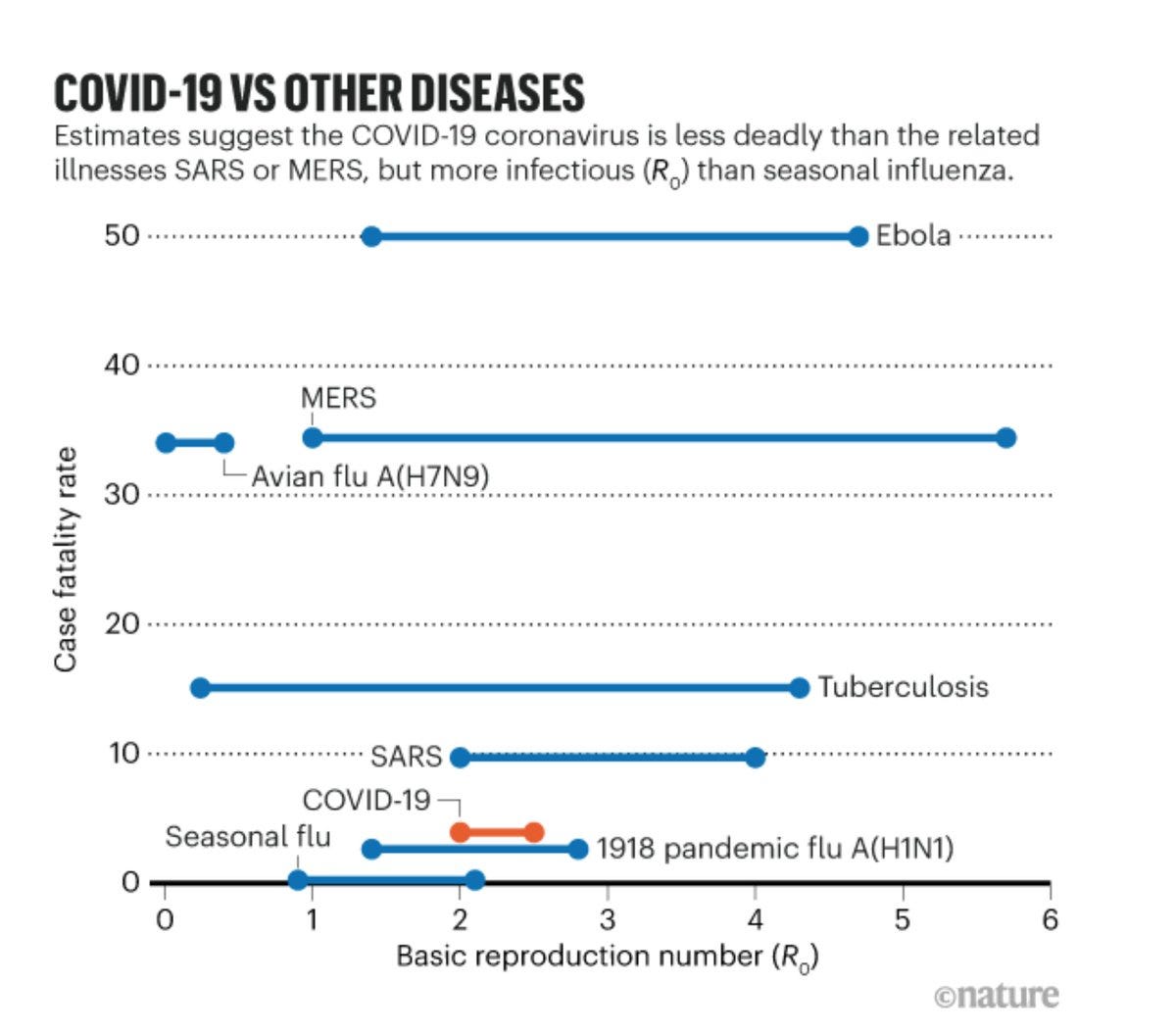
How Strong Is The "Viral Effect" Of Covid-19?
By "viral effect" we mean its ability to spread as measured by R-Nought. The short answer is, stronger than seasonal flu but less than other viruses:
While the true viral capacity is unknown at this moment, it is theorized that COVID-19 is more than the seasonal flu but less than other viruses. The average number of people to which a single infected person will transmit the virus, or Ro, range from as low as 1.5 to a high of 3.0
An Ro of 2.0 indicates that the virus could go exponential, so that's a real concern. Seasonal flu comes in around 1.3. Here's a nice graphic:
However, in the real world exponential growth always runs into logistic problems in maintaining that growth rate, so the growth rate tends to slow over time. Other concerns like the mortality rate then take over.
Asymptomatic Spread?
Probably vastly overrated:
“We still believe, looking at the data, that the force of infection here, the major driver, is people who are symptomatic, unwell, and transmitting to others along the human-to-human route,” Dr. Mike Ryan of WHO Emergencies Program.
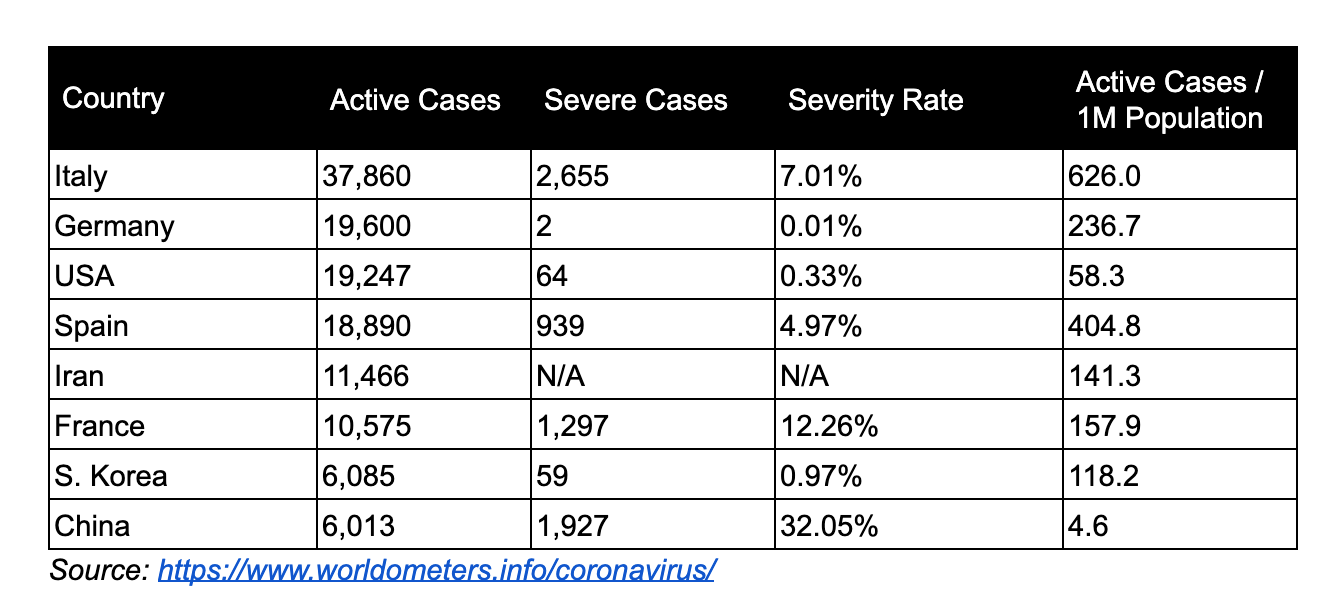
Rate Of Severe Illness?
Here's a nice graphic of the Chinese experience:
What will it be like in the US?
As of mid-March, the US has a significantly lower case severity rate than other countries. Our current severe caseload is similar to South Korea. This data has been spotty in the past; however, lower severity is reflected in the US COVID-19 fatality rates (addressed later).
Early reports from CDC, suggest that 12% of COVID-19 cases need some form of hospitalization, which is lower than the projected severity rate of 20%, with 80% being mild cases.
For context, this year’s flu season has led to at least 17 million medical visits and 370,000 hospitalizations (0.1%) out of 30–50 million infections. Recalling that only comparing aggregate total cases isn’t helpful, breaking down active cases on a per-capita basis paints a different picture on severity. This is data as of March 20th, 2020.
Two points here:
1. The flu season begins in September. Because flu does not spread as rapidly, doesn't achieve exponential growth rates, the case load is spread over many months. Note, too, that the hospitalization rate for all seasonal flu cases is much lower than that for Covid-19.
2. Thus we can see the importance of keeping overall Covid-19 numbers down--the overall case count. The reason for that is because if they grow rapidly in a shorter time period our hospital system will quickly be completely overwhelmed by the higher hospitalization rate.
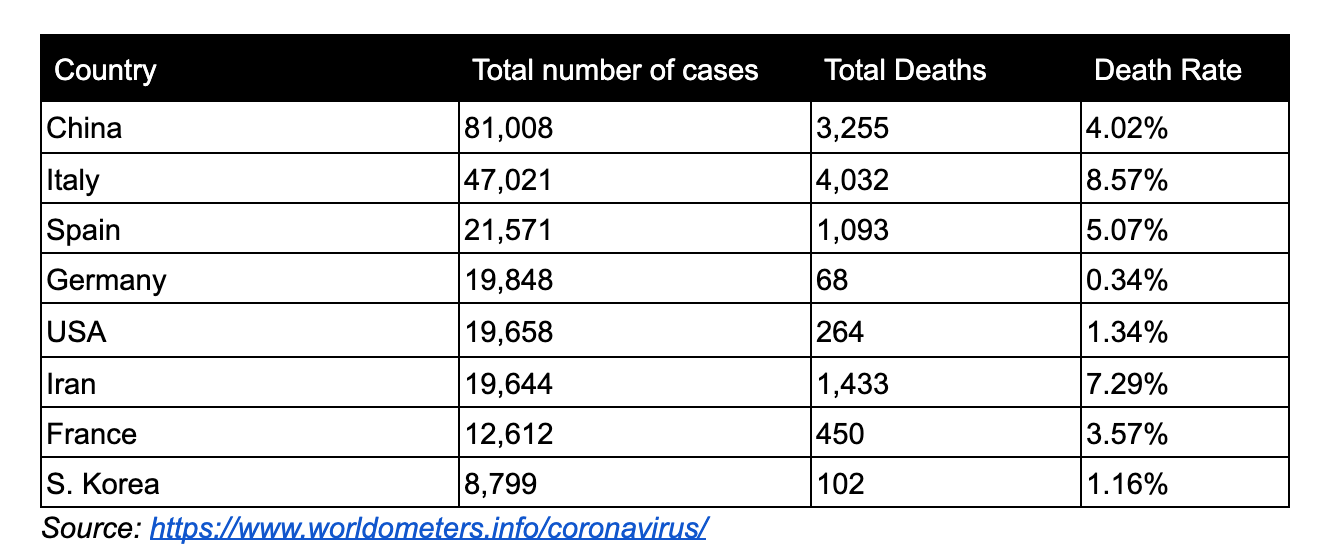
Mortality Rates
This is where the rubber meets the road. The good news is that right now the US is more comparable to South Korea than to European countries. OTOH, South Korea famously took very aggressive steps, which suggests that the US did the right thing. Also, the US onset of infection appears to have lagged that of the rest of the world. Again suggesting that this is probably not the time to let up.
Since there is a wide range of opinion on what the mortality rate will end up being, I'll just offer some interesting charts and comparisons. Note two things:
1. Mortality is by no means confined to the over-70 gang, and
2. The mortality rate does appear to be more severe than that of seasonal flu.
The Bottom Line
The bottom line as I see it is that Covid-19 is a very serious matter, but that infection is far from an inevitability. Handwashing is good, but it seems to me that mask-wearing is probably vastly underrated as a preventive step--at least in the US. The reason is obvious--the US is very much unprepared and simply doesn't have anywhere close to the number of masks of any sort that it should have. The good news, however, is that homemade masks are, by all accounts (on the interwebs) quite effective. Given that the predominant means of infection is droplets rather than an aerosolized mist, the effectiveness of mask wearing in even more underrated than we already think.
Perhaps this would be a good example of social distancing v. isolation. PA just reopened rest stops on the Turnpike to support truckers bring the rest of us food and other essentials. So they can eat, sleep, and take care of other vital functions.
ReplyDeleteAs reported to me by a friend who has a San Diego State retired professor of virology, masks are to prevent the wearer of the mask from touching his face and introducing the virus to his mouth or mucus membranes in the eyes and nose.
ReplyDeleteNo doubt there's truth in that. OTOH, people in places like HK, Taiwan, Korea, Japan mask up for other reasons. Their medical professionals are excellent, so I wouldn't want to dismiss their views. It might make a difference here.
DeleteWhy Wearing a Face Mask Is Encouraged in Asia, but Shunned in the U.S.
From The Guardian:
DeleteClaim: ‘Face masks don’t work’
Wearing a face mask is certainly not an iron-clad guarantee that you won’t get sick – viruses can also transmit through the eyes and tiny viral particles, known as aerosols, can penetrate masks. However, masks are effective at capturing droplets, which is a main transmission route of coronavirus, and some studies have estimated a roughly fivefold protection versus no barrier alone (although others have found lower levels of effectiveness).
If you are likely to be in close contact with someone infected, a mask cuts the chance of the disease being passed on. If you’re showing symptoms of coronavirus, or have been diagnosed, wearing a mask can also protect others. So masks are crucial for health and social care workers looking after patients and are also recommended for family members who need to care for someone who is ill – ideally both the patient and carer should have a mask.
However, masks will probably make little difference if you’re just walking around town or taking a bus so there is no need to bulk-buy a huge supply.
There is a frustrating amount of confusion about terminology. “Masks” are what medical personnel wear to protect their patients from infection. From the pictures I’ve seen out of Asia these are what most people are wearing. This makes sense as a measure to slow down the spread of the disease from people who may not even know they have the virus. But they are useless as protection for the wearer. A “respirator” (i.e., N95), on the other hand, DOES protect the wearer from infection if worn correctly. The two devices look similar and are made from the same materials but have very different designs and functions.
DeleteBro, are you sure you want to say "useless"? Don't you mean, "not as useful?" There are gradations here. The Guardian says a mask--meaning a surgical type mask, I'm sure--"cuts the chance." That sounds common sensical to me, just as the doctor says in the linked article about Asia. Doctors in Asia aren't stupid people. If a disease is often spread by droplets, any sort of barrier is bound to help.
DeleteYou’re right. Not useless. More like very limited since they don’t form a seal. But good at catching the germs coming out of the wearer. Also, they do tend to keep folks from touching their face, so there’s that.
DeleteI didnt mean to suggest anyone is stupid. If a mask is all you got, clearly you wear the mask. The docs really need the respirators, though, Hence Trump’s request that construction companies donate their supply. Back in mid-feb I went to Lowes to buy a few for when the SHTF. I bought the last few. Now that I know I won’t be using them, I will donate them to the local hospital. God help those folks in the weeks (months?) ahead.
DeleteI saw a comment stating that Taiwan (population 23 million) produces 70 million masks (unspecified) PER WEEK, but are willing to share 100K with the US per week. They believe strongly that masks are an essential part of inhibiting the spread of disease, as do other East Asian countries. It's hard to argue with their success.
DeleteIt looks like there is an organized campaign to denounce Aaron Ginn's article in the article's comments.
ReplyDeleteNot sure if it's organized. My purpose was to use the valid data that he offers, not to critique a very long article. He does actually say some rather stupid things. For example, it's apparent that he's never heard of the exponential curve v. the logistic curve--thus he thinks a slowing of an exponential growth rate is a sign to stop worrying. As I say, my purpose wasn't to critique him, so I just left that fairly lengthy section out. Also his recommendations, which IMO don't follow from the data but instead flow from his particular ideology.
Delete"The greatest shortcoming of the human race is our inability to understand the exponential function." Physicist Al Bartlett.
ReplyDeleteMasks would help by reducing the spread, unfortunately there are no masks available. Home Depot, Lowe’s, and Ace have been out for over a month in So Ca. If more masks were available in the us, more people would wear them.
ReplyDeleteIt’s amazing that Taiwan has been going business as usual, with mask wearing outside required. They did not restart their schools till there were enough masks.
The issue is the us just does not have enough masks, with the majority of factories overseas.
Hopefully Trump invoking DPA will help change that.
DeleteTwo quotes seem relevant, tossing them out for thought:
ReplyDelete"According to a study of the fatalities of COVID-19 cases in Italy, 99% of all deaths had an underlying pathology. Only 0.8% had no underlying condition."
"Most of those infected in Italy were over the age of 60, but the median age of a fatality was 80. All of Italy’s fatality under the age of 40 were males with serious pre-existing medical conditions."
Trump is destroying the economy of all for the sake of a sub-group (sick old men). Doesn't seem reasonable.
Who is the biggest beneficiary if everything crashes - China (and Dems).
I don't really know what he could have done differently, but he seems to be under the sway of socialists now (most health professionals like Fauci are leftists), who don't care about economics, as long as we save one more life, and he's not getting the good advice like he used to.
Well I'm one of those, "old sick men," when I'm not at my day job as a 'Boomer Rube', and I can remember a time when it was understood by pretty much everyone that had graduated at least 6th grade that reducing individual human value to a mere economic calculation was pretty much a core precept of Socialist ideology. There used to be many foolish old notions maintained by Western Civilization, like, I d'know, maybe those old fuddy-duddy Ten Commandments, and were considered 'reasonable'. Your possibly right, perhaps I have outlived my usefulness to the collective; yet, I persist.
DeleteTom S.
I think it's not really a question of "outlived my usefulness to the collective"
DeleteI'm going on 69 myself, altho without any known underlying conditions.
Nobody wants to die.
But at some point, isn't the question, do we sacrifice the economy for 330 million people, for the sake of how many thousands of deaths?
Almost 14,000 people died in 2009 swine flu, and not a word was said, and Obama did nothing for months.
I think that's why some are saying "Get people back to work and get the economy back under control while isolating and monitoring the old and infirm, all while utilizing best treatment options and continuing to look for a vaccine"
If that means spending billions to build hospitals in 2 weeks like China did, then do it.
Maybe better than wasting trillions by killing the whole economy.
Interesting take, from Ioannidis again:
ReplyDelete"...flattening the curve may make things worse: Instead of being overwhelmed during a short, acute phase, the health system will remain overwhelmed for a more protracted period"
https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/
I don't follow Ioannidis' 'reasoning' at all--because he provides no reasoning:
Delete"If the level of the epidemic does overwhelm the health system and extreme measures have only modest effectiveness, then flattening the curve may make things worse: Instead of being overwhelmed during a short, acute phase, the health system will remain overwhelmed for a more protracted period."
"If ... extreme measures have only modest effectiveness"
Exactly how does that work? Ioannidis grants that
"Flattening the curve to avoid overwhelming the health system is conceptually sound"
'Flattening the curve' through 'extreme measures' means 'social distancing'. It's been shown in the past to be the only thing that works short of specific medicines and vaccines--both of which we lack at this point (hope for chloroquine). Ioannidis admits this strategy is 'conceptually sound.' Why wouldn't that work in this case? Ioannidis doesn't share that with us. Social distancing means depriving the disease of new victims--how could that possibly not work to slow the spread down and allow for the health system to cope better? An unimportant detail for Ioannidis?
Exactly what is interesting to you about such bare assertions?
The clock is ticking. How much longer? The Deep State is putting gas into its tank.
DeleteCIA says they told Trump about the virus months before he acted. FBI says skinheads plan to weaponize the virus. No word yet on what #BLM is up to. Fauci on TV says it's going to be several weeks, if then, before Americans go back to their routines. The first suicides are starting.
The bond market is on life support. New York wants a bond bail out of the MTA. The MTA? How do you spell rot, corruption, crony capitalism and incompetence?
New York should not get one thin dime.
We've spent $2 trillion, so far. It did nothing. BigGov wants to spend trillions more. And they're lining up: airlines, Boeing, colleges.
Where is this money coming from?
If you are going to institute a policy, such as what we have done, then you accept the consequences. You don't do X and then in the middle of it try to stop its effects.
Putting a cordon sanitaire around New York, Chicago, some other big cities to stop the spread probably makes as much sense as what we are now doing to the entire country.
Ioannidis is simply paraphrasing Dickens, "If they're going to die then they should do it and free up a hospital bed for essential services such as 'trans'mogrification."
DeleteTom S.
@Titan 28
DeleteI agree that corruption is our biggest enemy here.
Re the disease, consider that the Italians were very slow to react. This morning we learn:
"Provincial mayors are sounding an alarm that the virus-related toll fails to reflect a spike in deaths in the general population among those who have not been tested. Last week alone, 400 people died in Bergamo and 12 neighboring towns — four times the number who died the same week the previous year, according to the Bergamo mayor’s office. Only 91 of those had tested positive for the virus."
Very interesting: Medium took down the Evidence Over Hysteria post. "Violation of the Rules."
DeleteDoes this mean that there was a concerted effort to bring the author and his post down?
I doubt it. I suspect the reason is because intelligent people saw how flawed his analysis of (valid) data was. As I said earlier, I left out some of the really stupid stuff--like, he kept talking about pandemics following a "bell curve," when he should have been talking about concepts he obviously had never heard of: exponential curve v. logistic curve. My purpose yesterday was to offer grounds for optimism in the big picture, not to take a deep dive and critique his long presentation. Others have done that, but I'm surprised at some of the uncritical gullibility of mainstream conservatives at prominent sites who don't even attempt to sepaate the wheat from the chaff in the article.
DeleteTrue enough. On a lighter note, I see that Mnuchin on TV said 'we're looking at a 10 to 12 week scenario' in the lockdown. Three months?
DeleteNope.
"Exactly what is interesting to you about such bare assertions?"
DeleteThe whole quote was "Flattening the curve to avoid overwhelming the health system is conceptually sound — in theory"
He goes on "if the health system does become overwhelmed, the majority of the extra deaths may not be due to coronavirus but to other common diseases and conditions such as heart attacks, strokes, trauma, bleeding, and the like that are not adequately treated. If the level of the epidemic does overwhelm the health system and extreme measures have only modest effectiveness, then flattening the curve may make things worse: Instead of being overwhelmed during a short, acute phase, the health system will remain overwhelmed for a more protracted period."
...
"One of the bottom lines is that we don’t know how long social distancing measures and lockdowns can be maintained without major consequences to the economy, society, and mental health. Unpredictable evolutions may ensue, including financial crisis, unrest, civil strife, war, and a meltdown of the social fabric."
In effect, There would be many people unable to get treatment for all the other problems that people go to hospitals for.
I have also seen a number of people arguing that it can't be contained, only mitigated.
I think his main push is that there is inadequate data to support the unprecedented "solutions" that government is pushing, and the effects will be worse than the disease.
It might be better to spend the money on medical facilities, to take care of those affected, and let the rest of the world go about it's business.
How many respirators and masks and hospitals can you build with 2 trillion dollars?
"The whole quote was "Flattening the curve to avoid overwhelming the health system is conceptually sound — in theory"
DeleteHey, FU. "conceptually sound" means the same thing as "sound - in theory." He was being redundant and I chose to shorten it.
or.. the concept is sound - in theory. Perhaps not exactly the same thing, depending on how you take it.
DeleteAnyway, I see you didn't respond to any actual point except to swear at me, so I'll withdraw.
Consider me surprised, and I won't be commenting further.
"you didn't respond to any actual point"
DeleteWhy would I respond to someone who wrongly accuses me of falsifying someone else's views? Or who suggests that instead of using the known workable strategy of social distancing we should start building new hospitals while the virus spreads like wildfire?
The fact is, I gave a detailed analysis of how Ioannidis avoids any justification of his claim that social distancing might not work. Instead of addressing my very specific critique you drop another excessively long comment on me and expect me to drop everything and answer things that I've already addressed. Sorry--my time is worth more than that.
A quibble:
ReplyDeleteMW wrote:
>>An Ro of 2.0 indicates that the virus could go exponential, so that's a real concern. <<
A clarification is needed at this point, I think, as I've seen this sort of comment a number of times. An Ro >1 means the disease starts to spread over time. All such spreading diseases have an exponential growth initially, as long as the initial R value is greater than 1. The difference is the larger the Ro value, the more rapid the exponential growth will be, initially. The early phases of the spread of a disease, though all are exponential, can often be difficult to distinguish from a linear growth rate, because the slope of the function isn't changing very fast in the early phase, and if there's noise in the data one might be tempted to fit it to a linear approximation, because it will fit that virtually as well as an exponential function, but since it is an infectious disease, the function describing the number of current infections is indeed exponential to start out with.
The thing that distinguishes low Ro infections from high Ro infections is the rate at which the current infections accelerate. High Ro current infections numbers accelerate much faster than low Ro numbers, though they are all on an initial exponential trajectory when they start.
Once the disease starts to spread, for Ro greater than 1, the % of the population that is not yet infected (or vaccinated) starts to decline, as people catch and recover from the illness (or get vaccinated). So the very exponential function that describes the growth rate of the current infections also defines the rate at which the segment of the population that cannot be reinfected grows (add to that all those getting vaccinated, which is not currently relevant to CV19)
Thus, the faster a virus infects others is also the rate at which the population of potentially infectibles at any give time is declining. This is why the virus that spread fast, dies out fast -- herd immunity rises with the same rate at which it spreads (minus deaths), as the population of uninfectibles grows and the infectibles % drops. This is characterized by the so-called instantaneous R value (without the zero subscript) which starts out at Ro but then decreases as the infection spreads; this is what decelerates the initial exponential growth rate to lower and lower rates of growth -- corresponding to lower and lower instantaneous R values until it reaches R=1.0, at which point the spread of the disease is no longer increasing (though additional people are still being infected, -- the re-infection rate is simple equal to the rate of recoveries at that point, and as the % of the population that is still infectible drops further, the R value drops below 1.0, and the current infection population function now has a negative slope, and the epidemic eventually dies out (technically the rate of re-infection may not go to zero, but attains a very low value.)
That's a somewhat oversimplified explanation. (The re-infection rates are also affected by social distancing, hygiene practices, vaccination programs, etc.) Also, the lower the Ro, the lower the % of recovered or vaccinated in the population needed for herd immunity to stop the growth in current infections.
The main point is all virulent disease with an initial Ro>1.0 will follow this exponential growth, deceleration, and decline in the rate of current infection, even if we do nothing.
Here's an article that may interest you, speaking in terms of network theory:
Deletehttps://www.zdnet.com/article/graph-theory-suggests-covid-19-might-be-a-small-world-after-all/
They also manage to explain what you said ... more briefly:
The point is that a lot of real-world networks, such as infectious disease, are not random networks where there is an even chance of any one person coming into contact with another. They have structure, and the dominant structure of those networks is that the vast majority of people have a sparse number of connections to local neighbors. A random network would imply exponential growth, whereas the so-called scale-free networks that Barabási discovered do not. (If you want to dig into more about small-world networks, with excellent illustrations of how things propagate, especially disease, check out an excellent paper written by noted researcher Valdis Krebs, who is chief scientist with Orgnet, LLC.)
Something like what Barabási discussed is identified in the Ziffs' paper. There is a tapering off that's been seen in the China data, they write, after an initial exponential curve. That suggests to them a "kind of small-world interaction network where individuals have many local neighbors and occasional long-range connections (such as caused by people traveling on trains, boats, and planes)."
The practical implication, if their model is correct, is that the speed of the disease is taking longer and longer to double in the number of deaths. Exponential growth is not maintained because "the number of susceptible individuals around an infected individual decays with time," as a result of the prospect that "Individuals already infected might face increased immunity and there are other individuals who might have had a mild infection that imparts immunity but without developing symptoms warranting testing."
"These various effects would inhibit the exponential growth of the virus."
It would seem that the majority of the spread would have to be from asymptomatic carriers despite the encouraging article above. Common sense and my own experience has been that no one hangs around anyone who is hacking or sneezing, not since we became aware of this in February. The numbers of infections just seem way too high for casual contact or the negligence of people when in groups. I have heard very compelling evidence on both sides of these questions. I prefer the distancing. Even with a 0% mortality, this would have crippled the world with its severity for the 10-20% would are health comprimised.
ReplyDeleteThe quote in my comment above may bear upon what you're saying. It deals with networks in the real world. The infection travels through networks of people, and if those networks don't intersect the disease transmission is stopped. The hard part is maintaining that, which means locating the ill and treating them. As you say, distancing is key, and it's NOT just a theory.
DeleteTwo comments:
ReplyDelete1 I wish all the Anonymous and Unknown people here would take about one minute to think up a screen name, or just use their real name, or whatever, and sign in, so that people (like me) who frequent this place can keep you all straight!
2 I've been reading what everyone has to say about the trillions, and flattening the curve, and just going back to work, and how its not the flu, and the greater evil, and, really everything. Its a fascinating debate and I'm going to keep reading and trying to think it all through.
But I just have this nagging concern that (even with all the information I get here) I don't have all the facts, and I am not a government official, let alone a leader, nor am I a doctor or a public health expert...in fact, I am probably not all that smart a guy! So where I come out is that, for better or for worse, I'm going to look to the President to do the right thing and cross my fingers that he does and will.
Then there will come a day when the score is totalled up and we'll see how he did. I'm not saying to y'all don't keep researching and debating...I'm just saying I'm going to go with some old-fashioned trust...at least for the time-being.